PhD Research
Positron emission tomography (PET) is a nuclear medicine diagnostic imaging exam of metabolic processes in the body. PET performance and image quality degrade as patient body size increases due to poorer acquisition statistics. Recently available time-of-flight instrumentation and image reconstruction methods for PET will, theoretically, improve the quality of raw data and reconstructed images for larger patients (diameter >20 cm). The long-term goal of my project is to measure TOF and non-TOF PET image quality for a range of sizes, a variety of radioactivity distributions, and a variety of attenuation distributions.
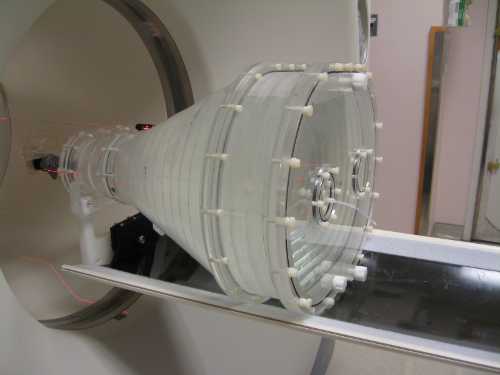
To measure PET scanner performance and image quality over a wide range of sizes, a novel fillable, tapering phantom (i.e., a plastic container that can be repeatedly filled with radioactivity and scanned) was designed and built. The phantom's diameter ranges from 17 to 44 cm over a length of 31 cm and has a mass of 42 kg when filled with water. To approximate cancerous lesions and measure image quality, 1.0-cm spheres were filled with a sphere-to-background radioactivity concentration (18F-FDG in water) of 8:1 and positioned throughout the phantom's volume. A 1.0-cm size sphere is a useful metric because it is at the edge of lesion detectability for current PET scanners. Using these lesions with this phantom, the image quality improvement of time-of-flight over conventional PET has been parameterized as a function of body size. A multisphere phantom (below), analysis algorithms, and a fillable, tapered phantom (left) that have already been developed will be good tools for evaluating image quality improvements using TOF PET compared to non-TOF PET as a function of size. With additional simulations and acquisitions, the phantoms will be validated as tools for measuring a continuum of cross-sectional dimensions in PET imaging.

As a result of my research, I am able to take a circumspect approach to designing phantoms for image quality measurements that considers PET system and processing parameters including: sensitivity, spatial resolution, count rate, and reconstruction. Having authored and modified image analysis algorithms I am able to manipulate image formats (e.g., DICOM, raw sinogram) and work with several coding languages (e.g., C, Bash, MATLAB, Perl). Along with image analysis algorithms, I have a general understanding of Monte Carlo software features, and a specific working knowledge of the SimSET Monte Carlo software.

I have participated in multiple PET/CT phantom studies and system performance testing on the Duke PET Facility's GE Discovery ST, STE, and 690 PET/CTs. Thus, I am capable of drawing dose, acquiring images with the routine "clinical interface" on the scanner, reviewing and analyzing images, using the system's research tools, and manipulating system files that allow: changing energy thresholds, modifying acquisition and reconstruction protocols, and writing scripts that measure system performance. I have authored and implemented QC and PET acquisition protocols that are routinely used in our clinic.
Science INTERESTS
Evidenced-based Medical Imaging Practices
One of the certainties that exist in the health care industry today is that the future of finances in the health care industry in uncertain. How will uninsured Americans have their health care needs met? How will insured Americans be covered? How will the overhead of the medical industry be paid for? At what level and through what mechanisms will physicians be reimbursed? Who will pay for all of this?
In any realm of health policy or regulation (e.g., reimbursement, approval for use in humans, research funding) nuclear medicine and molecular imaging must always address at least three criticisms: cost, radiation exposure, and outcomes. The instrumentation, siting, and support of nuclear medicine departments have both high initial and ongoing costs compared to other health services. During the debates and public discourse of the PPACA, medical imaging was often singled out as cause for increased medical use and cost. A dramatic increase in the number of imaging studies, applications, and equipment was commonly used as a surrogate for arguing excessive costs and over-utilization, though not explicitly stated. It is certainly true that access to imaging systems and the number of studies has grown rapidly in the last two decades, but assessing the efficacy of an imaging test is difficult because they are diagnostic and not therapeutic.
The medical imaging scientific and academic community can, and must continually, address these criticisms. In terms of health policy and regulation as it applies to our profession, we must first police ourselves. There have been steps taken to reduce costs and radiation dose, but more can be done by reducing unnecessary repeat studies and increasing electronic medical records and reporting. Additionally, we must be ahead of the curve in moving from anecdotal to evidence-based decision-making. At a time when medical cost are being questioned, we must have evidence that by changing the clinical decision we are either improving the patient population's outcome or reducing the net cost of treatment.
Science Communication
I am passionate about the importance of effective science education and communication; experts and leaders in the medical field are expected to serve, and are often funded by, the public. Thus, I believe there is a duty to communicate with and educate all audiences (e.g., patients, clinicians, physicians, policy makers, fellow researchers). I believe that the nature of my research goals necessitates a bi-directional, healthy relationship with clinical practice. Good communication and education within hospital departments and across the professional community are essential for the optimum application of current technologies as well as the integration of new techniques and equipment.
While I have been in Graduate School, one of the "hard-skills" that I've worked at developing (aside from my research) is being a good scientific/technical writer. I am not an expert by any stretch of the imagination, and there is always more to learn. I have organized and collaborated with Medical Physics students to host two Medical Physics Scientific Writing Seminars (Summer 2007, Spring 2010). For the set of seminars, I compiled and authored a brief guide to writing scientific abstracts.